How to Calculate Insulin Doses: The 500 Rule and 1800 Rule Explained
This calculator estimates mealtime (bolus) and correction insulin doses using two formulas that are widely taught in diabetes education: the 500 Rule for figuring out an insulin-to-carb ratio, and the 1800 Rule (or the 1500 Rule for regular/short-acting insulin) for figuring out an insulin sensitivity factor. These rules were popularized by diabetes specialists as practical starting points and are commonly referenced in diabetes self-management education programs.
Important: This tool is for educational and reference purposes only. Insulin needs vary significantly from person to person based on body weight, activity level, insulin type, illness, medications, and many other factors. Never start, stop, or change an insulin dose based on this calculator alone — always work with your doctor, endocrinologist, or diabetes care team to set and adjust your actual ratios and doses.
Understanding the Formulas
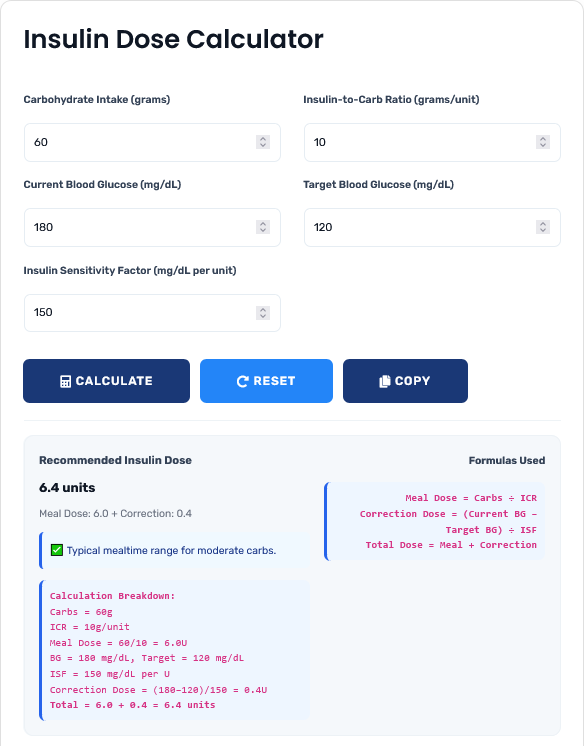
Meal (Bolus) Dose = Carbohydrates (g) ÷ Insulin-to-Carb Ratio (ICR)
Correction Dose = (Current Blood Glucose − Target Blood Glucose) ÷ Insulin Sensitivity Factor (ISF)
Total Dose = Meal Dose + Correction Dose
What Each Term Means
- Insulin-to-Carb Ratio (ICR): How many grams of carbohydrate are covered by one unit of rapid-acting insulin. A common starting-point estimate is the "500 Rule": divide 500 by your total daily insulin dose (TDD) to get an approximate ICR.
- Insulin Sensitivity Factor (ISF), also called a "correction factor": How much one unit of insulin is expected to lower blood glucose, measured in mg/dL. A common starting-point estimate is the "1800 Rule" (for rapid-acting insulin) or the "1500 Rule" (for regular insulin): divide 1800 (or 1500) by your total daily insulin dose.
- Target Blood Glucose: The blood glucose level you and your care team have agreed you're aiming for before meals, typically set individually.
- Total Daily Dose (TDD): The sum of all basal and bolus insulin a person typically uses in one day.
These "rules" produce starting estimates, not final answers. Actual ICR and ISF values are set and refined by a healthcare provider based on blood glucose logs, HbA1c trends, and individual response. Many people's real ratios differ meaningfully from what the 500/1800 rules suggest.
Insulin "Stacking" and Insulin On Board
Rapid-acting insulin stays active in the body for a period of time after it's taken — commonly several hours, though the exact duration depends on the insulin type and the individual. This remaining active insulin is often called "insulin on board" (IOB). If a correction dose is calculated without accounting for IOB from a previous dose, it can lead to "stacking" — effectively taking more insulin than intended — which raises the risk of hypoglycemia (low blood sugar).
This calculator does not currently factor in insulin on board. If you've taken a dose recently, talk to your diabetes care team about how to safely account for it before calculating a new correction dose.
Why Getting This Right Matters
Insulin dosing sits at the intersection of two risks: too little insulin allows blood glucose to run high over time, which is linked to long-term complications, while too much insulin can cause hypoglycemia, which can be dangerous quickly. Because of this, small arithmetic mistakes matter more with insulin than with most other medications — this is one reason diabetes educators encourage using a calculator or double-checking mealtime math rather than estimating by hand, especially for people newer to carbohydrate counting.
Special Situations That Change Insulin Needs
Insulin sensitivity and requirements are not fixed — they commonly shift with:
- Illness or infection: the body often needs more insulin during sickness, even with reduced food intake.
- Pregnancy: insulin resistance changes throughout pregnancy and typically requires frequent dose review with a provider.
- Physical activity: exercise can increase insulin sensitivity for hours afterward.
- Certain medications: steroids, for example, are widely known to increase insulin resistance; some other medications can lower insulin needs. Always review your full medication list with your provider.
- Kidney or liver function: impaired clearance can change how long insulin stays active in the body.
- Growth (in children/teens): insulin needs typically increase as children grow, particularly during puberty.
Anyone in these situations should work closely with a healthcare provider rather than relying on standard ratios.
Related Calculators
For broader health tracking, you may also find these useful: our blood pressure calculator, heart rate calculator, and the full health calculators collection.
Frequently Asked Questions
The 500 Rule is a common starting-point method for estimating an insulin-to-carb ratio: divide 500 by your total daily insulin dose (TDD). For example, if your TDD is 50 units, 500 ÷ 50 = 10, suggesting roughly 1 unit of insulin covers about 10 grams of carbohydrate. This is only a starting estimate — your actual ratio should be confirmed and adjusted by your healthcare provider.
The 1800 Rule estimates your insulin sensitivity factor for rapid-acting insulin by dividing 1800 by your total daily dose. The 1500 Rule is the equivalent formula used for regular (short-acting) insulin. Both give an estimate of how many mg/dL your blood glucose is expected to drop per unit of insulin.
The math itself (carbs ÷ ICR, and (current BG − target BG) ÷ ISF) is simple arithmetic and will always be correct given the numbers you enter. What can't be guaranteed is that your entered ICR, ISF, and target values are the right ones for your body — those need to come from your healthcare provider and be reviewed periodically.
No. This calculator is designed for mealtime (bolus) and correction doses of rapid-acting insulin only. Basal insulin dosing follows different principles and should be set by your healthcare provider.
Children, teens, and pregnant women often have insulin needs that change frequently and require closer medical supervision than the standard formulas assume. Please use this tool only alongside guidance from a pediatric or obstetric diabetes care team in these situations.
No, it does not currently calculate insulin on board (IOB). If you've taken insulin recently, ask your diabetes care team how to factor that in before taking an additional correction dose, to avoid stacking insulin.